Product Overview
Indications for Use
Related Documents
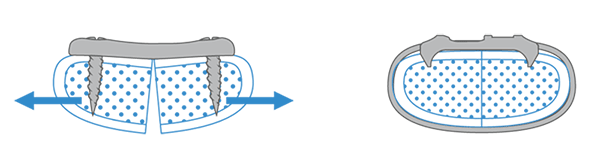
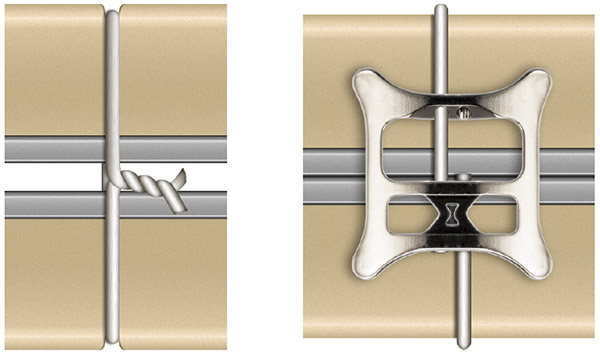
Greater Stability
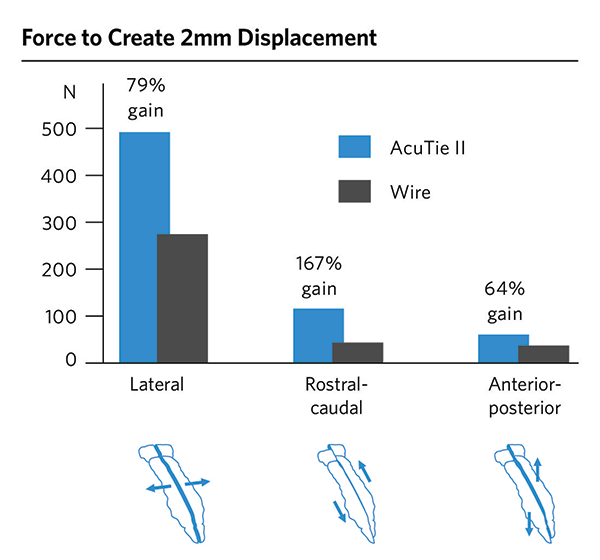
Resists motion in all three planes – lateral, rostral-caudal, anterior-posterior.
AcuTie II plates and wire cerclage were installed on foam blocks and loaded in all three planes until 2 mm of displacement was created.
AcuTie II outperformed wire significantly in all three planes.1
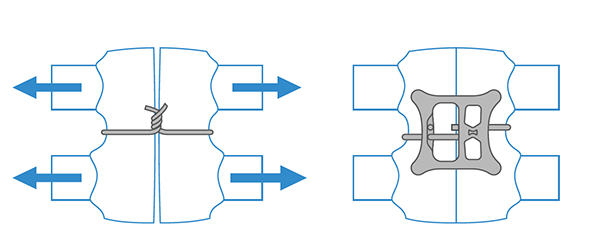
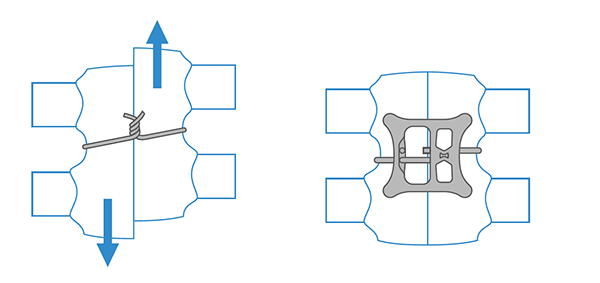

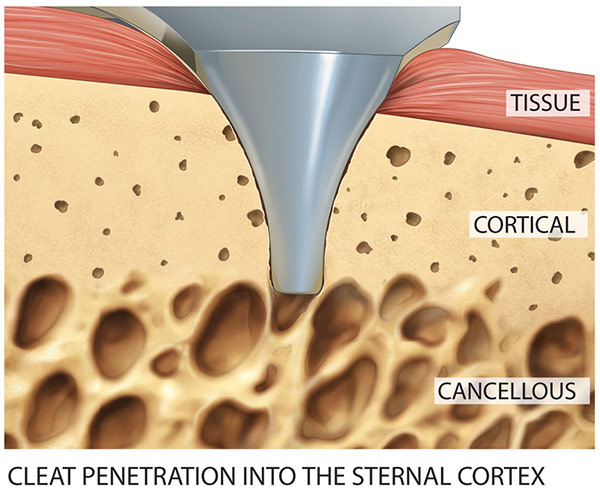
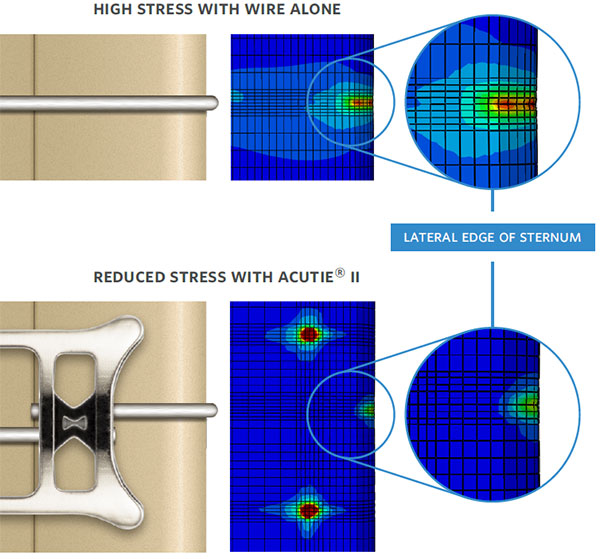
Lateral Protection
Directional cleats assist with distributing the load and reduces stress on lateral edges.
Directional cleats penetrate through soft tissue and into the bone for stability, like a screw, while distributing the load and reducing stresses on the lateral edges of the sternum.
Like barbs, they allow medial movement of the sternum halves during reduction and gripping during distraction.
Twisted wire and AcuTie II plates were installed on simulated foam sterna with 20 pcf (cortical) exteriors and 5 pcf (cancellous) interiors.
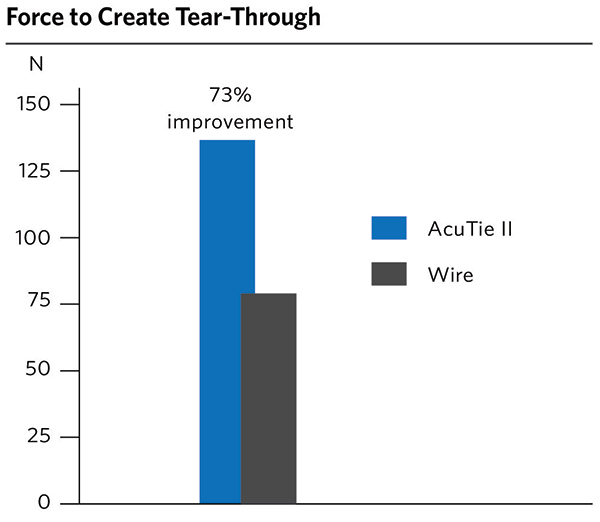
The sternal halves were pulled laterally and the force to tear through the bulk of the sample was measured. AcuTie II could resist 73% more force than wire alone.1
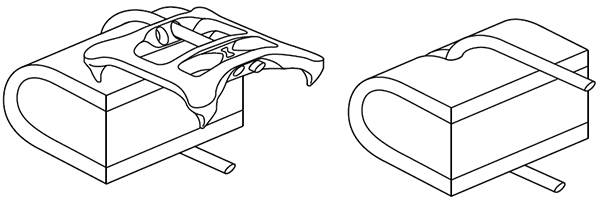
A finite element analysis shows how load is distributed via the cleats from the lateral sternal edges to the anterior table of the sternum.
Testing shows a 73% increase in the force needed to tear through when compared to wire alone.1
Easy Installation
- Plate installs in less than 90 seconds.1
- Quick, repeatable installation.
- Confident re-entry without specialized instrumentation.

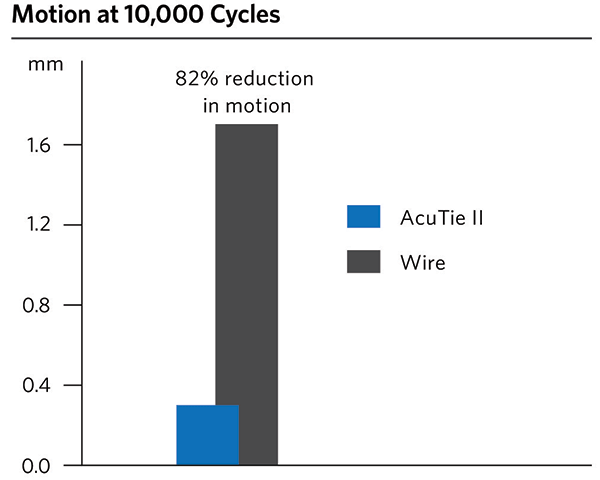
Cyclic Performance
The AcuTie II plate experienced approximately 82% less motion than twisted wire.1
The plate’s crimp feature eliminates fatigue and breakage caused by twisted and bending wire. At coughing forces, a twist will typically break within 20,000 cycles. An AcuTie II crimp will survive more than 200,000 cycles.1
The crimp, combined with the other system features, results in significantly improved cyclic performance.
AcuTie II plates and twisted wire were installed on 30 pcf foam blocks and loaded from 0 to 200N for 10,000 cycles. 60% of twisted wires broke prior to reaching 10,000 cycles. The average AcuTie II plate sample experienced approximately 82% less motion than twisted wire.1
Cost-Effective
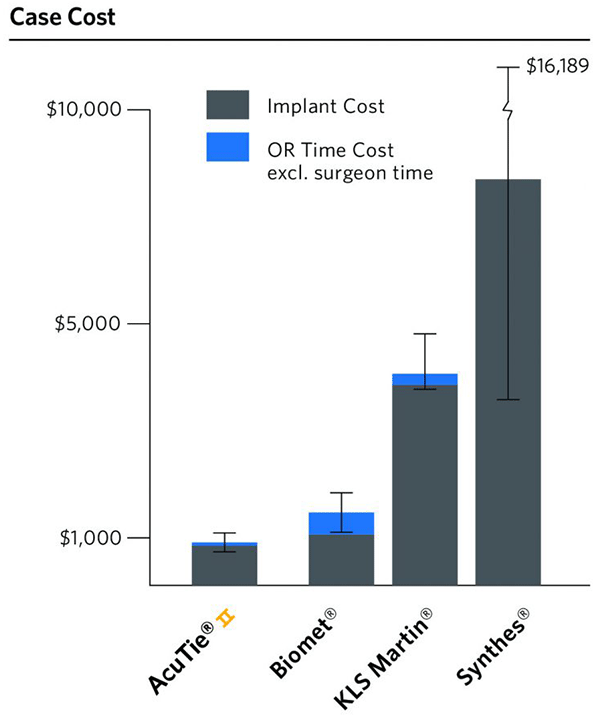
Other plating options can cost $1,480 to $8,508 per case depending on the system, number of implants used, and the additional OR time needed for installation.2,3,4,5
An AcuTie II plate can be installed in less than 90 seconds using standard sternotomy wire and minimal instrumentation.1
Locking plate systems can take more than 15 minutes to install.4 In addition to longer anesthesia time, and at a hospital cost of approximately $25/min, excluding surgeon time,5 this can translate to significant added cost.
High cost may make some options prohibitive for routine use, even when limited to patients at high risk for DSWI.
AcuTie II Sternum Closure System Surgical Lab and Technique Overview
Citations
- Data on file at ACUTE Innovations.
- Huh J Bakaeen F, Chu D, Wall MJ. Transverse sternal plating in secondary sternal reconstruction. J Thorac Cardiovasc Surg. 2008 Dec 1;126(6):1476-80.
- Levin LS, Miller AS, Gajjar AH, Bremer KD, Span n J, Mialo CA, et al. An Innovative Approach for Sternal Closure. Ann Thorac Surg. 2010 Jun:89(6):1995-9.
- Song DH, Lohman RF, Renucci JD, Jeevanandam V, Raman J. Primary sternal plating in high-risk patients prevents mediastinitis. Eur J Cardiothorac Surg. 2004 Aug 1;26(2):367–72.
- Stahl JE, Sandberg WS, Daily B, Wiklund R, Egan MT, Goldman JM, et al. Reorganizing patient care and workflow in the operating room: a cost-effectiveness study. Surgery. 2006 Jun;139(6):717–28.